")
")
")
Despite the overwhelming majority of R&D, regulatory, sales, marketing, and corporate finance focus in the advanced wound care (AWC) sector being on physical advanced wound care products, many of the greatest opportunities to drive outcomes–and profitability–exist in the realm of wound care service delivery.
This concept was further developed by senior management from several of the leading global AWC brands in the well-received executive panel session we facilitated in Gothenburg, Sweden earlier this year at the EWMA Conference. Keeping with this theme, several of the speaking engagements, articles, partnership explorations, and related advisory we have performed towards the end of this year have revisited this idea. We will share some areas of particular interest below.
Calling all forward-thinking AWC professionals
Whether you’re in AWC or an adjacent sector (dialysis, diabetes, vascular, ortho, plastics, home care, etc.), or affiliated with a service provider and/or payer organization (ACO, IDN, HMO, CCG, VA)…if you’re seeking to partner with like-minded, forward-thinking executives, payers, health systems / facilities, clinicians, and investors on the types of initiatives discussed in the remainder of this article, get in touch to describe your unique approach and what you and your colleagues stand to gain and could bring to the table. We’ll confidentially use this to explore if there are existing or future collaboration opportunities to accelerate your goals within the Diligence Wound Care Global network.
When you have the wound care “Hardware,” but what you need is the “Software”
This concept was eloquently articulated a couple of years ago by one of our Singaporean clients…During a tour of several large, well-equipped, generously-staffed, high volume wound care facilities in several countries as part of the early experience program, he witnessed firsthand the lack of administrative support, uniform processes, data analytics, and relative ability to influence key (external) decision makers among the potential customer sites.
Immediately after one such customer visit, he turned to me and exclaimed, “They have plenty of ‘hardware,’ but what they need is ‘software!’”
In addition to the educational and networking opportunities, we had the opportunity to contribute as faculty at The Association for Advanced Wound Care (AAWC)’s track at The 2019 Desert Foot Multi-Disciplinary Limb Salvage Conference in Phoenix, Arizona earlier this month. One of the topics, Bringing Together Best-in-Class Clinical, Operational, and Technological Approaches to Delivering Advanced Wound Care: An Interactive Panel Discussion, leveraged live polling of the AWC clinicians and administrators in attendance to draw attention to some very surprising yet highly relevant and underappreciated stakeholder pain points and related market needs.
Barriers to adoption of new products and technologies
Firstly, if you were to ask the average commercial or medical affairs AWC (or more broadly speaking, medtech) professional about the key activities needed to gain adoption, they would likely list the following product-centric factors among their top three replies:
- Presenting and communicating scientific and clinical evidence
- Education and training of staff
- Initial trialing and feedback
Strikingly, the live polling results as articulated by actual AWC users and customers suggest exactly the opposite, with their top three barriers overwhelmingly being:
- [Navigating] administration and bureaucracy
- Financial pressures to always choose the cheapest or on-contract option
- Logistics (too many supplies to order, stock, etc.)
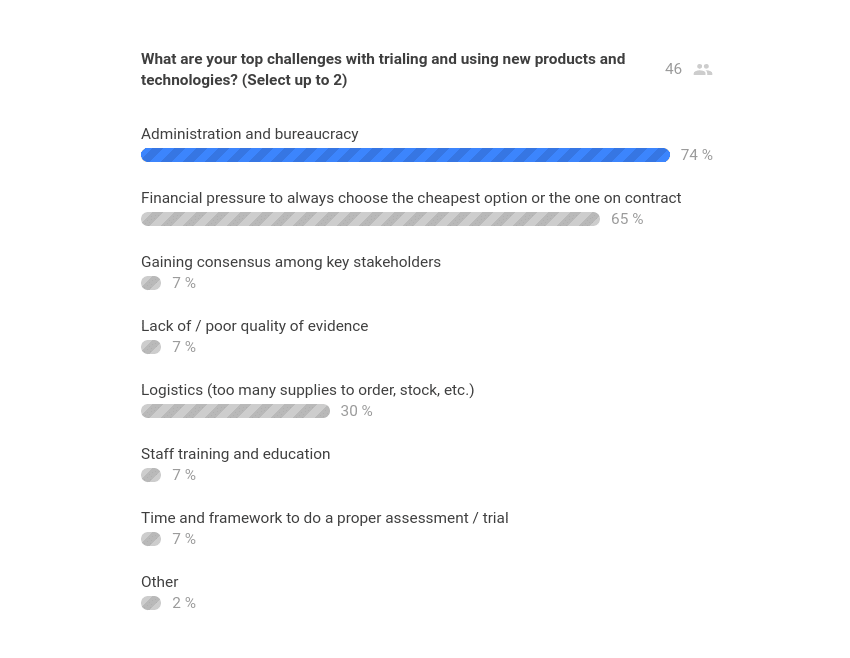
The audience-reported feedback is consistent with our experience as both an AWC customer and strategist, and is equally as relevant in the non-US markets as it is in the US.
Stated differently, even when discussing a topic such as adoption of new AWC products, the key barriers are ironically related to services (management, administration, logistics, etc.).
This concept was eloquently articulated a couple of years ago by a Singaporean client, a seasoned global marketing executive in the midst of a best-in-class product pre-launch across nine Asian markets. During a tour of several large, well-equipped, generously-staffed, high volume wound care facilities in several countries as part of the early experience program, he witnessed firsthand the lack of administrative support, uniform processes, data analytics, and relative ability to influence key (external) decision makers among the potential customer sites.
Immediately after one such customer visit, he turned to me and exclaimed, “They have all of the ‘hardware,’ but what they need is ‘software!’” The phrase stuck with us throughout that engagement and beyond, anytime we encountered care delivery that was inconsistent, inefficient, unscalable, or otherwise not meeting its full potential despite adequate physical resources (in other words, the vast majority of AWC facilities and providers) . In fact, improving stakeholders’ “software” for delivering care then became a critical parallel activity alongside the traditional “hardware” sales and marketing activities during the actual launch phase, with major dividends in terms of building customer trust and branding for the distributor and their products alike.
Clearly, the misalignment on AWC “hardware” (tangible facilities, products, and staffing) vs. “software” (intangible processes, protocols, tech, analytics, business/financial models, and other enablers) is something holding the sector back from its full potential on a global scale–and thus represents a phenomenal opportunity for non-AWC and AWC firms alike.
Barriers to adoption of digital health (mobile assessments, diagnostics / imaging, telemed, analytics, etc.)
Another highly instructive live audience poll from the event specifically zoomed in on the top barriers to adoption of digital health (literal “hardware” and “software,” not to be confused with the figurative “hardware” and “software” described above). The results are here:
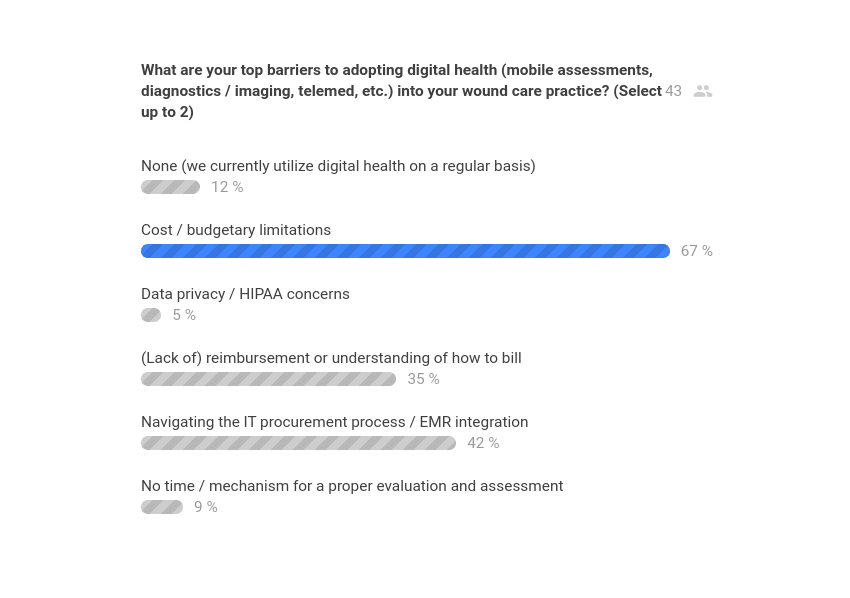
Once again, just like with physical product adoption, the most pressing challenges to adoption of digital health faced in the real world are overwhelmingly managerial, administrative, and financial in nature. This begs the question: Why do so few digital health initiatives in AWC actually address these gaps?
One might even argue that the majority of AWC digital health creation and marketing activities are not even taking aim at the right problems to solve. But even putting that point aside, can these issues of how to secure budgeting, viable business / financial models, and integrations (both technical and practical) be effectively tackled by individual corporations and health systems alone? At what point does there need to be more cross-pollination beyond just the AWC industry?
As payers, adjacent / complementary service lines, and non-AWC (and even non-healthcare) tech firms (such as consumer electronics) become more involved in the AWC sector, the pace of not only innovation, but also adoption, of wound care digital health is likely to accelerate sharply. The convergence of demographic, epidemiological, healthcare economics, and overall awareness trends will further fuel these drivers as well.
The panel’s perspective
With a podiatric surgeon / the conference co-chair (Anthony Tickner), a wound and ostomy nurse practitioner (Emily Greenstein), a wound specialist physical therapist (Renee Cordrey), and a wound care strategic advisor / wound care center executive (Rafael Mazuz) comprising the panel, the perspectives were (almost!) as insightful as the actual live audience polling and questions.
On the topic of best practices for (figurative) “software,” Dr. Tickner discussed the incorporation of standing orders and similar processes for standard of care assessments, diagnostics, and in some cases product applications, routine interventions, and interdisciplinary consultations.
Ms. Cordrey and Ms. Greenstein also discussed how evolving payment models and new technologies are incentivizing and making it easier than ever for wound care clinicians “to practice to their full scope.” They provided examples such as nursing staff providing certain physical therapy services and physical therapists providing certain wound care services–with the ability to connect to educational resources, asynchronous, and even live clinical expertise to improve the quality of care and reduce the waste and other costs associated with sending multiple clinicians on separate care visits.

The new Patient-Driven Payment Model (PDPM) and Patient-Driven Groupings Model (PDGM)
We are seeing this trend play out right before our eyes. In conjunction with the new CMS Patient-Driven Payment Model (PDPM in the US), which is focused on skilled nursing facilities (SNFs) and went live on October 1, 2019, Genesis Healthcare, Inc. (NYSE:GEN) laid off 585 rehab employees (nearly 6% of the total). In the two months since the announcement, the Genesis Healthcare stock price has risen by over 50%.
The home healthcare equivalent of PDPM is called Patient-Driven Groupings Model (PDGM), which is scheduled to go live on January 1, 2020. The new system is actually expected to materially raise average wound care reimbursements in the home health setting, but like PDPM disincentivizes higher utilizations of clinical and product resources.
Needless to say, PDPM and PDGM are significant developments for care settings where a material amount of wound care takes place–both individually and collectively. The most astute product and services firms have already begun to capitalize on these and related needs, and access to remote expertise via telemedicine is a prime example:
Unlocking and securing budgetary, staffing, equipment, and other resources
Another dimension of AWC presenting a substantial opportunity has to do with rallying the appropriate resources and growth plan for a new or existing wound care program.
In late September, we published a post on the AAWC blog, entitled, “Unlocking Resources for Wound Care Teams: Tips for Demonstrating Value.” The piece laid out a simple step-by-step plan involving:
- Determining baseline metrics and KPIs (key performance indicators)
- Ensuring a proper organizational and financial structure
- Using a dashboard report to regularly share (in person) with institutional administration
In the December issue of Today’s Wound Clinic, our article focused on the often elusive wound care budget and related financial literacy for wound care providers in, “An Introduction To Understanding, Articulating, and Managing Your Wound Clinic’s Finances.”
To the professional investors, healthcare administrators, product executives, and anyone else with P&L responsibility reading this, it might seem like an overly simple read. Resist the urge to skip over it. Rather, refer back to the survey results above: The primary drivers of customers passing up your products, technologies, and other solutions are due to the lack of (perceived) administrative and financial knowledge, tools, and other resources. While the content of the TWC article was aimed at clinicians and others lacking formal business, economics, or financial training, the need to bridge this gap is something that stakeholders at all levels of AWC (and adjacencies) should be acutely concerned with.
We culminated the exploration of financial and administrative approaches to wound care with a second presentation at this year’s Desert Foot conference, entitled, Strategies and Tactics for Gaining Support from Management to Secure Wound Care Resources for You, your Team, and your Patients.
The session essentially focused on how to raise the bar for AWC management (administrative and clinical alike) to elevate a new or existing program to the same level of rigor and “seriousness” in the eyes of senior administrators and payers, who are typically not wound care experts, yet control the majority of funding, staffing, and other resources that go into a successful hospital department, clinic, home care, or other program.
Click here for the full event interaction report.
Future AWC opportunities: Don’t miss your seat at the table!
Are you part of a healthcare services firm and/or payer focused on advanced wound care (or an adjacency), curious about how / with whom to partner in order to optimize your model with clinical-operational efficiencies and digital technologies?
A medtech or biotech products firm interested in diversification into services?
An angel investor, venture capitalist, hedge fund, private equity, or other investment professional / firm who would like to know where the promising plays are in this space?
Contact us today to discuss.